STOP Adverse Drug Reactions From
Taking Their Toll on Your Residents
…and Your PROFITS!
The Right Drug
The Right Dose
Right From The Start
Covered by Medicare and Medicaid*
How Much Are ADRs Costing
Your Facility?
Adverse Drug Reactions (ADRs) are the most expensive and clinically significant drug-related issue in long-term care settings today1.
The average facility – with 105 beds – experiences 135+ ADRs annually1, costing tens of thousands of dollars.
ADRs demand more staff hours, hiking labor costs and, because most facilities bill on a fixed monthly rate, this added cost is squeezed out of the facility’s already-strained bottom line.
Fast Facts
Every year, nursing homes report over 350,000 ADRs.2
22% of Medicare beneficiaries experience an ADR during their SNF stay, 59% of which are “likely preventable.”3
1 in 10 long-term care residents experience an ADR within 30 days of admission.1
ADRs increase ER admissions by as much as 42%, and 30-day hospital readmissions by a staggering 52%.4
ADRs are linked to skin ulcers, agitation, loss of appetite, impaired thinking, and loss of balance causing falls and other injuries.
Given the astronomical number of deaths, ER visits, hospitalizations and suffering attributed to preventable ADRs, it’s astonishing most doctors continue to practice the “one-size-fits-all” approach to prescribing drugs.
1NIH-National Institutes of Health. 2FDA- Food and Drug Administration. 3Department of Health and Human Services. 4John Nelson, MD., former president of AMA.
Save Money and Improve the Quality of Life for Your Residents
Medicare and Medicaid* now cover a non-invasive, genetic test that reduces the risk of ADRs.
With a simple cheek swab, doctors can learn if a drug is more likely to help or harm a patient – before he/she even consumes the drug.
Without PGx testing, doctors must put their patients through riskydrug trials,costingfacilities significant amounts of money – while subjecting their patients to ineffective medications and insidious side effects before finally finding a drug that works best.
Remarkably, most physicians are not up to speed with this innovative technology and unwittingly dismiss the test as a time constraint, at the patient’s and facility’s expense – thus, many people needlesslysuffer from preventable ADRs.
*Medicaid in approved states
Not All Pharmacogenetic (PGx) Test Are Created Equal
It is essential to mention that most labs focus on only a limited number of drugs, genes, and variants, so many physicians have never been exposed to
an efficacious test. This has led to some hesitation among doctors in implementing PGx tests.
An efficacious PGx tests utilizes Next Generation Sequencing (NGS) assay to provide clinically actionable information for medications across a broad
range of medical fields, including anesthesiology, cardiology, endocrinology, gastroenterology, gynecology, immunology, infectious diseases,
neurology, oncology, pain management, psychiatry, respiratory, rheumatology, toxicology, urology, and more.
The test also yields results for drug-drug, drug-food, drug-alcohol, and drug-lab interactions.
*Typically, test results take about ten days, so preemptive testing is highly recommended so the results are readily available in a medical emergency or before trying a new drug.
Aligning Rx with DNA and LTC Communities
For Communities
Saves Time and Money
Pharmacogenetics aligns current and future medications with each resident’s unique genetic profile.
It was designed to help clinicians determine the right drug, at the right dose, for the right person.
In a community setting, pharmacogenetics can be utilized to address clinical concerns such as:
It enables personalized therapeutic decisions for people suffering from some of the most prevalent clinical conditions including, Cardiovascular Disease, Neuropsychiatric Disorders and Pain.
For Residents
A Better Quality of Life
Have you ever been told to take a medication for a few weeks and see if it works?
It’s a guessing game and you continue to guess until you start feeling better, or worse. This can take weeks,
months, even years as you suffer through side effects, pain and sometimes adverse events from medications that don’t work.
Pharmacogenetics is a simple test that will help your healthcare team provide better “personalized” care and treatment options. The pharmacogenetic test is a simple swab of the cheek that is 100% reimbursed by Medicare B and in some states, Medicaid.
The goal of personalized medicine is to streamline clinical decisions and avoid the “trial and error” process that providers have been using for so many years.
Benefits of PGx and Personalized Medicine
More Informed Prescribing Decisions
Saves Time
Saves Money
Reduces ER Visits
Reduces Hospital Readmissions
Reduces Mortality Rates
Reduces Pain & Suffering
Enhances Safety Measures
Achieve Therapeutic Benefits Sooner
Lifetime Utility
Covered by Medicare and Medicaid*
*Medicaid in approved States
Leading Medical Institutions That Have Adopted PGx Testing
St. Jude Children’s Hospital tests all its patients stating,
“If you knew about this genetic information and didn’t act on it, you would not be practicing good medicine.”
Financial Cost and Consequences of
“Trial and Error” Prescribing
Real People- Real Cases - Real Proof - Real Cost
Marion W.
Marion was PGx tested in April 2019. Based on the results, her doctor advised her to stop taking the Metoprolol, which she had been taking for years, and decreased the dosage of her HBP medications. Two years later, her pain management doctor ignored her PGx report and prescribed 300 mg of Tramadol, which caused a life-threatening ADR, and she was hospitalized for three days. If her doctor had adhered to the PGx report guidelines, all the expense and suffering could have been avoided.
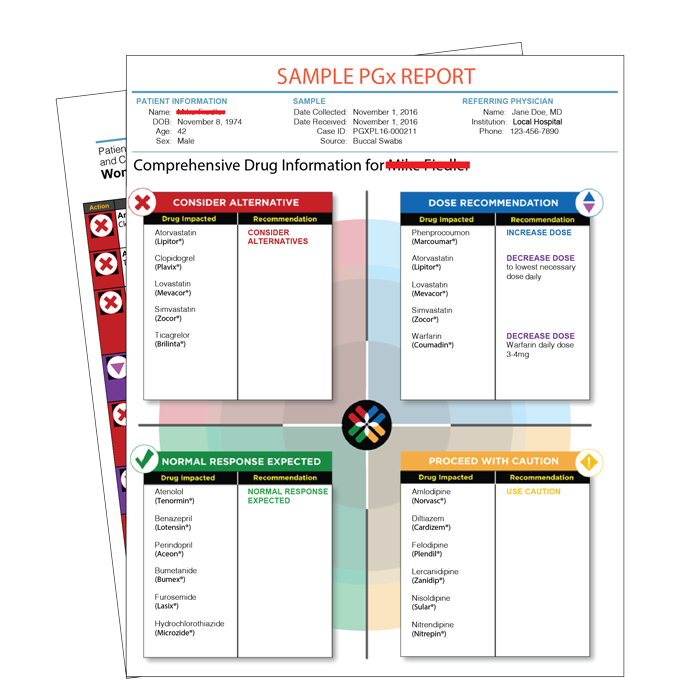
Mike F.
Mike was having difficulty sleeping, so his doctor prescribed Escitalopram. After five weeks of undesirable side effects and no relief, he had a PGx test and learned he was a rapid metabolizer of Escitalopram. If he had been preemptively PGx tested, it would have saved him and his insurance company money and Mike time by avoiding a useless trip to the pharmacy to purchase an ineffective drug. More importantly, he would have received relief weeks sooner.
Dorothy J.
Dorothy was experiencing a piercing headache, so she went to the ER. They gave her Reglan 5mg, IV push once, and Toradol 15 mg. A few days later, she had stroke-like symptoms, so her doctor ordered an MRI. Several months later, she had a PGx test and discovered that she was a slow metabolizer of Toradol. If she had a preemptive PGx test, it could have saved her insurance carrier thousands of dollars and spared her the distress and anguish caused by a preventable ADR.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}